

Introduction
Monoclonal gammopathy of undetermined significance (MGUS) is a premalignant clonal disorder, which progresses at a rate of 1% per year to multiple myeloma (MM), or other plasma-cell or lymphoid disorders. MGUS is common and occurs in approximately 3% and 5% of persons 50 and 70 years of age or older, respectively. Clinical factors reported to be associated with MGUS progression include MGUS isotype, abnormal serum free light-chain ratio (FLCr), and high serum monoclonal protein (M protein) level (>=1.5 g per deciliter). Body mass index (BMI) has also been seen associated with MGUS progression, but has not been evaluated in context of established clinical prognostic factors. Here, we evaluate the contribution of BMI to MGUS progression beyond clinical prognostic factors in a population-based study and examine differential associations by sex.
Methods
We studied 594 patients residing in Olmsted County Minnesota, who were identified with MGUS in a screening study conducted between1995 through 2003. Patients with light-chain MGUS were not included. Patients were screened for M-protein [normal (<1.5 g/dl) or high (≥1.5 g/dl)], FLCr [normal (0.26-1.65) or abnormal (<0.26 and/or >1.65)], and isotype (IgG, IgM, IgA, bi-clonal). Follow-up time was calculated from date of MGUS screening to date of last follow-up, death, or progression to MM or another plasma-cell or lymphoid disorder. BMI (kg/m2) was calculated using height and weight values reported close to sample date (80% of patients within 2 years), and then categorized into BMI<25 and BMI≥25. We used Cox regression to estimate the association of BMI with risk of MGUS progression to MM or another plasma-cell or lymphoid disorder, univariately, and accounting for clinical factors. Analyses were also stratified by sex. We report hazard ratios (HR) and 95% confidence intervals (CI).
Results
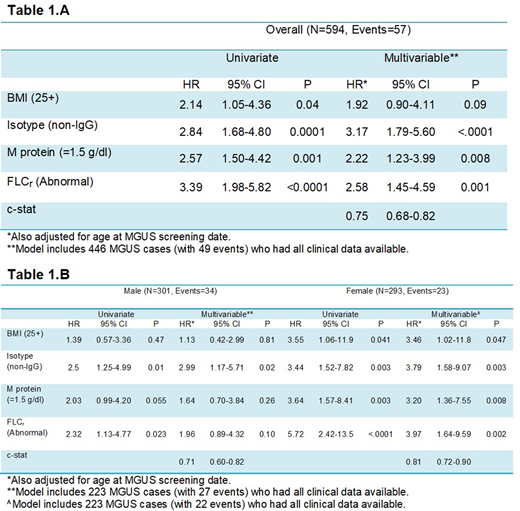
Of the 594 patients, 51% were male, and the median age at screening date was 73 (range:50-98 years). The immunoglobulin type was IgG in 71% of patients, IgM in 17%, IgA in 10%, and bi-clonal in 2%. High M protein level was observed in 22% and abnormal FLCr in 28%. BMI≥25 was observed in 67% of patients. The median follow-up time was 10.5 years (range:0-25). Over a median of 6,846 person-years, 465 patients (78%) died and 57 patients progressed and developed MM (N=39), amyloidosis (N=8), lymphoma (N=5), or Waldenstrom macroglobulinemia (N=5). The overall rate of progression was 0.87 events (CI:0.67-1.12) per 100 person-years, and higher among males (1.01, CI:0.73-1.42) than in females (0.72, CI:0.48-1.08), however, the difference was not statistically significant (P=0.24). In univariate analyses, BMI≥25 (HR=2.14, CI:1.05-4.36, P=0.04), non-IgG isotype (HR=2.84, CI:1.68-4.80, P=0.0001), high M protein (HR=2.57, CI: 1.50-4.42, P=0.001), and abnormal FLCr (HR=3.39, CI:1.98-5.82, P<0.0001) were associated with increased risk of progression (Table 1.A). These four factors were independently associated with MGUS progression in a multivariable model, with a c-statistic=0.75 (CI:0.68-0.82). When stratifying by sex, associations of BMI with progression were stronger among females than males (Table 1.B) [c-statistic=0.81 (CI:0.72-0.90) vs 0.71 (CI:0.60-0.82) for females vs. males respectively], however, a test for interaction between BMI and sex was not statistically significant (P=0.15).
Conclusions
In this study we found evidence that high BMI is a prognostic factor independent of isotype, M protein, and FLC ratio in the full cohort, however, this was mainly driven by the effect in females rather than males. Future studies should further investigate sex differences in evaluating prognostic factors among MGUS patients.
Dispenzieri:Intellia: Research Funding; Pfizer: Research Funding; Alnylam: Research Funding; Takeda: Research Funding; Celgene: Research Funding; Janssen: Research Funding. Kumar:Genentech/Roche: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Cellectar: Other; Kite Pharma: Consultancy, Research Funding; Tenebio: Other, Research Funding; BMS: Consultancy, Research Funding; Karyopharm: Consultancy; MedImmune: Research Funding; Sanofi: Research Funding; Celgene/BMS: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Janssen Oncology: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Amgen: Consultancy, Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments, Research Funding; Merck: Consultancy, Research Funding; Adaptive Biotechnologies: Consultancy; Genecentrix: Consultancy; Takeda: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Dr. Reddy's Laboratories: Honoraria; AbbVie: Other: Research funding for clinical trials to the institution, Consulting/Advisory Board participation with no personal payments; Novartis: Research Funding; Carsgen: Other, Research Funding; Oncopeptides: Consultancy, Other: Independent Review Committee; IRC member.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal